There is wide variation in the structure and function of the different types of endogenous molecules which act as signal transmitters, from tiny gasses such as nitric oxide and carbon monoxide (sometimes referred to collectively as gasotransmitters), through neurotransmitters to peptide hormones and growth factors. In the Peptides section we provide information relating to the different families of peptide hormones, mediating a wide variety of signals responsible for controlling many essential biological processes. In this section we provide information related to important ‘other’ types of endogenous signaling molecules.
Some signaling molecules are small molecules which bind to cell surface receptors to modulate a signalling cascade and others are able to cross the cell membrane to exert their effects intracellularly. Signalling by these mediators can be by endocrine, paracrine or autocrine mechanisms.
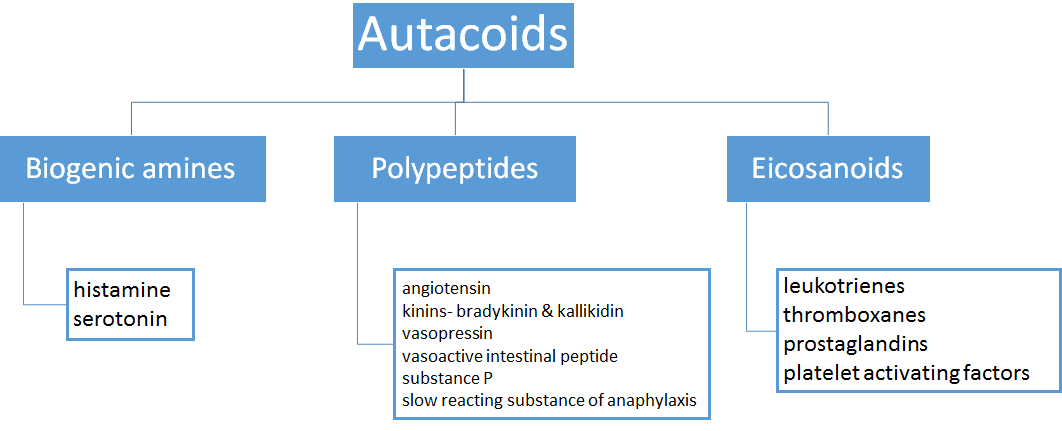
Gasotransmitters, neurotransmitters, steroid hormones and eicosanoids are all examples of endogenous cell signaling molecules.
Gasotransmitters
There are many gaseous chemicals with effects/functions in the human body, however only three of these act as bona fide ‘gasotransmitters’ (or gaseous transmitters): nitric oxide (NO, a free-radical mediator), carbon monoxide (CO) and hydrogen sulfide (H2S). These three regulate a variety of key biological functions and are also implicated in tumour biology. They can have endocrine, paracrine, and autocrine actions. They are produced enzymatically under tight regulation. They have varying biological half-lives, which affects their mode of transmitter action. NO has a very short half-life (seconds) restricting it to autocrine or paracrine action. H2S survives for seconds to minutes, and CO has the longest half-life, maintaining activity for several minutes.
Nitric oxide is biosynthesized from the substrate L-arginine, using oxygen, and NADPH by various nitric oxide synthase (NOS) enzymes. Reaction products are L-citrulline and NO. The three NOS enzymes are neuronal NOS (nNOS), inducible NOS (iNOS) and endothelial NOS (eNOS). As their names suggest nNOS is primarily expressed in the brain and neuronal tissue and eNOS is expressed predominantly in the endothelial layer of the vasculature. These two isoforms show subcellular localisation. They are both constitutive, low-output enzymes. This is in contrast to high-output iNOS which shows largely cytosolic expression in immune cells such as macrophages. In normal physiology, NO binds to the haem group of guanylyl cyclase to increase intracellular cyclic GMP levels, with downstream effects resulting from modulation of cGMP-dependent protein kinases (PKGs). It also opens ATP-dependent potassium channels and mediates S-nitrosylation based protein modifications. Adverse effects of supra-normal levels of NO include inhibition of mitochondrial enzymes and initiation of DNA damage.
Endothelial NO: NO in the endothelium has a potent vasodilatory effect. Nitroglycerin (glyceryl trinitrate) is converted to nitric oxide in the body, hence its vasodilatory action. The NO moiety of the vasodilating antihypertensive drug minoxidil may act as a NO agonist, explaining some of its molecular mechanism of action.
Neuronal NO: Whilst mainly expressed in central and peripheral nervous tissue, nNOS is also found tethered to dystrophin in skeletal muscle. In these tissues NO acts as a classical transmitter enabling cell communication.
Immune cell NO: iNOS in monocytes, macrophages, and neutrophils can be activated by proinflammatory cytokines such as interferon-gamma (IFN-γ) and tumor necrosis factor (TNF). In contrast, transforming growth factor-beta (TGF-β) potently inhibits iNOS. iNOS-derived NO is used to regulate inflammation and immune responses to pathogens. The large quantities of NO produced in response to proinflammatory cytokines facilitates reaction with superoxide to form toxic peroxynitrite, as part of the macrophage oxidative burst. iNOS is also expressed in the cardiovascular system, but its role in these tissues is less clear.
Modified arginine analogues are inhibitors of all three isoforms, with different analogues exhibiting different inhibitory profiles. For example L-NNA is selective for eNOS and nNOS over iNOS.
Carbon monoxide is produced endogenously by the haem oxygenase enzymes (HO1 and HO2), as a product of oxidative degradation of haem. Expression of HO1 is induced by factors including haem, oxidative stress, UV radiation, heat shock, hypoxia and NO. HO2 is constitutively expressed in the brain, kidney, liver and spleen. At low physiological concentrations CO has antiinflammatory, antiproliferative, anti-apoptotic and anticoagulative responses. Like NO, CO also binds to the haem group of guanylyl cyclase, albeit with lower affinity than NO. CO also activates ATP-dependent potassium channels, and activates kinase signalling pathways (e.g. the PI3K–AKT and p38 mitogen-activated protein kinase pathways). At high concentration CO displaces oxygen from haemoglobin causing hypoxia (CO poisoning). CO can also inhibit mitochondrial cytochrome c oxidase (the last enzyme in the respiratory electron transport chain), at least in vitro, which may contribute to CO poisoning.
Hydrogen sulphide is a physiological modulator of blood pressure in humans. It is produced by the action of several hydrogen sulphide synthesis enzymes. It activates ATP-dependent potassium channels to mediate vascular smooth muscle relaxation. H2S in the CNS is implicated in Alzheimer’s disease, epilepsy, stroke and Down’s syndrome. Pharmacological enhancement of H2S levels may provide beneficial effects against gastric ulcer and in inflammatory bowel disease. Chattopadhyay et al. (2016) have reported the beneficial effects of a hybrid molecule combining naproxen with NO- and H2S-releasing properties in preclinical animal models, as a potential mechanism for overcoming the gastrointestinal limitations of naproxen use.
RESOURCES
This is a useful resource for those wishing to keep up to date with current literature in the field of gaseous transmitters. It is also a good place to find out about upcoming conferences in the subject.
This is a link to a set of articles published in the British Journal of Pharmacology as a special themed issue highlighting important discoveries in gasotramsmitter research.
Histamine
Histamine is a vasoactive amine (a.k.a. a biogenic amine). It acts via a family of G protein-coupled receptors (histamine receptors H1-H4). The histamine receptors are differentially expressed, and couple to different second messenger systems. This results in context-specific effects in response to histamine release.
HIstamine is produce from the amino acid histidine by the action of histidine decarboxylase. If not stored, it is rapidly inactivated by histamine-N-methyltransferase or diamine oxidase.
As an inflammatory mediator, histamine is released from storage granules located in connective tissue mast cells, basophils and eosinophils. IgE-sensitized cells degranulate when exposed to antigen. This stimulates release of stored histamine in to the surrounding tissues, where it promotes capillary permeability allowing leukocytes and immune reaction mediators access to local tissues. Histamine is the most significant mediator of pruritus.
In anaphylaxis, the histamine surge causes extensive vasodilation which results in a rapid reduction in blood pressure.
In nasal mucous membranes, histamine release causes increased vascular permeability which in turn allows fluid egress from the capillaries to surrounding tissues producing the allergic symptoms of a runny nose and watery eyes. Sneezing associated with allergy is caused by histamine-induced stimulation of sensory neurons in the nasal cavity.
Histamine is also involved in regulating physiological function in the gut where it is produced in the enterochromaffin-like (ECL) cells of the stomach. It acts locally on the histamine H2 receptor on parietal cells to increase gastric acid secretion. Antagonism of H2 receptors is the molecular mechanism of action of the antacids famotidine and cimetidine.
Lastly, histamine is know to have neurotransmitter activity. Histaminergic neurons in the tuberomammillary nuclei of the posterior hypothalamus project throughout the brain. Histamine signals from these cells control a variety of processes including arousal, learning, memory, sleep and energy balance, with histamine notably increasing wakefulness and preventing sleep. This is why older brain-penetrant antihistamines (antagonists targeting the H1 receptor) cause drowsiness. Histamine in the CNS is principally degraded by histamine-N-methyltransferase.
Mastocytosis is a mast cell activation disorder characterised by a proliferation of mast cells and excess histamine release. Sufferers of this condition are prone to itching, hives, anaphylactic shock and excess gastric acid production. In rare cases the disease is aggressive and can result in organ failure related to mast cell infiltration. Some patients develop malignant mast cell leukemia, and mast cell sarcoma. Symptomatic relief is multi-targeted: antihistamines, mast cell stabilisers, proton pump inhibitors, epinephrine, beta 2 agonists, corticosteroids, antidepressants and calcium channel blockers all target the various symptoms of the condition, but it cannot be cured. Intensive (chemo)therapy (with or without allogeneic stem cell transplantation) is considered in cases of malignant mast cell disease. Current and future treatment options are reviewed by Molderings et al. (2016) PMID: 27132234.
Neurotransmitters
Synaptic transmission relies on local synthesis, and release of neurotransmitter molecules at the synapse, binding of the neurotransmitter to its cognate post-synaptic receptor(s) and inactivation/removal of the neurotransmitter from the synaptic space to terminate the activation. Neurotransmitter inactivation is achieved by several mechanisms, including diffusion away from the synaptic space, enzymatic degradation (e.g. acetylcholinesterase which breaks acetylcholine) and reabsorption into the pre-synaptic terminal (e.g. reuptake of the monoamines by the selective reuptake transporters for dopamine, serotonin and noradrenaline).
Neurotransmitters act via ionotropic receptors and/or metabotropic receptors. Ionotropic receptors are ion channels to which the neurotransmitter binds directly, to modulate channel opening. Metabotropic receptors are ion channel associated G protein-coupled receptors which bind the neurotransmitter molecule facilitating indirect modulation of ion channel activity.
Neurotransmitters can be either excitatory or inhibitory in action.
Inhibitory neurotransmitters include serotonin, GABA and dopamine. Depending on context dopamine can be both excitatory and inhibitory. Serotonin is discussed in its own separate section below.
GABA (gamma-aminobutyric acid) acts via GABAB receptors (a pair of subunits which form a dimeric G protein-coupled receptor) which couple to ion channels, and ionotropic GABAA receptors (ligand-gated ion channels). GABA action contributes to motor control, vision and many other cortical functions, such as anxiety regulation. Epilepsy and Huntington’s disease tremor are two conditions treated by drugs which increase central GABA levels.
Dopamine acts via a family of G protein-coupled receptors. Activation of dopamine receptors is involved in controlling movement and posture. Loss of dopamine in specific areas of the brain causes the muscle rigidity typical of Parkinson’s disease. Dopamine analogues are used to re-establish physiological levels of dopamine to treat Parkinsonism. Dopamine also plays a central role in positive reinforcement and dependency, drive and motivation and is required for focus. Stimulants such as ADHD medications and caffeine mediate dopamine release at the synapse, thereby improving focus and attention span. It should be noted that prolonged stimulation can lead to dopamine depletion. Dopamine is also a chemical precursor required for the synthesis of epinephrine and norepinephrine.
Excitatory neurotransmitters include acetylcholine, glutamate, and the catecholamines dopamine, epinephrine and norepinephrine.
Acetylcholine is a very widely distributed excitatory neurotransmitter that triggers muscle contraction and stimulates the excretion of certain hormones. In the central nervous system, it is involved in wakefulness, attentiveness, anger, aggression, sexuality, and thirst. It acts via a family of muscarinic acetylcholine receptors (mAch receptors).
Glutamate binds to an orthosteric binding site on G protein-coupled receptors of the metabotropic glutamate receptor family (mGlu receptors) which transmit the signal to ionotropic glutamate receptors. It is a major excitatory neurotransmitter associated with memory and learning.
Epinephrine (adrenaline) acts via alpha- and beta-adrenoceptors (G protein-coupled receptors) to regulate heart rate and blood pressure. Epinephrine levels can be reduced in response to long-term stress or insomnia, and can be elevated in ADHD.
As a neurotransmitter norepinephrine (noradrenaline) is required for attentiveness, emotions, sleeping, dreaming, and learning. Low levels of norepinephrine are associated with low energy, decreased ability to stay focussed and sleep cycle problems. Elevated norepinephrine can cause anxiety and low mood. Norepinephrine also acts in the circulatory system to cause vasoconstriction and increased heart rate.
Stress, poor diet, neurotoxins, genetic predisposition, drugs (prescription and recreational), alcohol and caffeine can all reduce neurotransmitters to suboptimal levels.
Other neurotransmitters: aspartate (an excitatory amino acid), glycine (an inhibitory amino acid), histamine, adenosine and adenosine triphosphate (ATP) are all thought to have some neurotransmitter function. Peptides such as substance P, beta endorphin, enkephalin, somatostatin, vasopressin, prolactin, angiotensin II, oxytocin, gastrin, cholecystokinin, thyrotropin, neuropeptide Y, insulin, glucagon, calcitonin, neurotensin and bradykinin may also exhibit some neurotransmitter-like activities, or more likely act as neuromodulators affecting the the synthesis, breakdown, or reabsorption (reuptake) of neurotransmitters. The gasotransmitter NO, acts as a signalling molecule at synapses, passing between cells by passive diffusion.
Other autacoids
The pharmacology and clinical impact of histamine and serotonin have been described above. This section will focus on other clinically important autacoid molecules.
Autacoids release can be triggered by agents including chemical and immune irritants, UV light, bacterial toxins and physical trauma.
Whilst histamine mediates the wheal, flare and redness reactions, the prostaglandins mediate pain.
Autacoids antagonists include the antihistamines (see the Histamine section above), serotonin antagonists (see the Serotonin section above) and prostaglandin synthesis inhibitors (typically aspirin, paracetamol and the NSAIDs- see the Cyclooxygenase (COX) inhibitors section of the Enzymes module).
Eicosanoids
These are lipid derived molecules synthesized from arachadonic acid (AA). AA is liberated from membrane phospholipids by the action of phospholipase A2 (PLA2). The enzymes involved in the turnover of the eicosanoids can be viewed here.
Therapeutic uses of prostaglandins
PGE1 (alprostadil) is administered by intracavernosal injection to both diagnose and treat erectile dysfunction.
The synthetic prostaglandin analogue misoprostol has antisecretory and protective properties, promoting healing of gastric and duodenal ulcers. Used to treat benign gastric and duodenal ulceration and NSAID-associated ulceration. Misoprostol also acts as a potent uterine stimulant, and can be used off-label for termination of pregnancy (following mifepristone administration).
Leukotrienes
As their name suggests these agents are produced by leukocytes, but are also found in other immune cells. Leukotrienes act in a paracrine or autocrine manner to regulate immune responses and production is typically accompanied by secretion of the other inflammatory mediators, histamine and prostaglandins. Leukotrienes are divided in to two groups: the cysteinyl leukotrienes (LTC4, LTD4, LTE4, LTF4) which contain a cysteine residue in their structure, and the others which don’t have this cysteine residue (LTB4, LTG4 and LTB5).
Hyper-production of LTD4 is an important cause of airway inflammation in asthma and allergic rhinitis, and can induce anaphylactic shock. LTD4 is an agonist of the GPCRs CysLT1 and CysLT2. This action stimulates proinflammatory activities such as endothelial cell adherence and chemokine production by mast cells. The Leukotriene receptor antagonists montelukast (non-selective) and zafirlukast (CysLT1 selective), block the effects of cysteinyl leukotrienes in the airways. They are effective in asthma when used alone or with an inhaled corticosteroid. Leukotriene receptor antagonists may be of benefit in exercise-induced asthma and in patients with concomitant rhinitis.Tthey are less effective in patients with severe asthma who are also receiving high doses of other drugs.
Platelet activating factor (PAF)
PAF is synthesized by host defense cells (e.g. platelets, neutrophils, monocytes and macrophages) at constant low levels and in larger amounts by activated inflammatory cells (e.g. mast cells, eosinophils, basophils). PAF production (principally from the phospholipid, phosphatidylcholine) activated by inflammatory agents is thought to be the primary source of PAF under pathological conditions and is the source of the elevated PAF levels associated with allergic reactions, sepsis, colitis and multiple sclerosis. PAF antagonists would negate downstream effects of activation of the PAF receptor. Rupatadine is a dual histamine H1/PAF receptor antagonist approved in many countries for the treatment of allergic rhinitis and chronic idiopathic urticaria, but it is not available in the US.
PAF is also produced by renal mesengial and medullary cells and vascular endothelial cells. In the cardiovascular system PAF is a potent vasodilator. In the stomach it is a potent ulcerogen.
Thromboxanes
The two major thromboxanes are thromboxane A2 and thromboxane B2. The platelet enzyme thromboxane-A synthase converts prostaglandin H2 to thromboxane, and the thromboxane activates the G protein-coupled thromboxane A2 receptor, or TP receptor. Thromboxane is a vasoconstrictor, a potent hypertensive agent, and it facilitates platelet aggregation. In particular, thromboxane A2 produced by activated platelets is prothrombotic, activating new platelets and increasing aggregation.
Thromboxane inhibitors can be either synthesis inhibitors, or thromboxane receptor antagonists.
Aspirin and naproxen are synthesis inhibitors. Low-dose, long-term aspirin use irreversibly blocks the formation of thromboxane A2 in platelets, thereby reducing aggregation and providing the anticoagulant effect useful in reducing the incidence of heart attacks. High-dose naproxen induces near-complete suppression of platelet thromboxane without causing the cardiovascular hazard associated with high-dose use of other NSAIDs.
Ifetroban (Phase II clinical candidate drug), dipyridamole and terutroban (Phase III clinical trial terminated by the manufacturer) are thromboxane receptor antagonists. Dipyridamole exhibits a multi-faceted mechanism of action, inhibiting thromboxane A2 synthesis via inhibition of platelet phosphodiesterases, directly inducing prostacyclin release and antagonising the effect of thromboxane A2 at the TP receptor.
Picotamide is an investigational dual synthesis inhibitor and thromboxane receptor antagonist which has not reached the clinic. See Modesti et al. (1994) and Neri Serneri et al. (2004) for further details.
Retinoids
Retinoic acid (RA) is a metabolite of vitamin A (retinol). It promotes growth and development, controls anterior/posterior patterning in early embryonic developmental stages and is necessary for spermatogenesis in humans.
Retinoic acid activates the RAR retinoic acid receptors and RXR retinoid X receptors. These are nuclear hormone receptors.
Retinoic acid analogues are used in oncology and dermatology. Because of the importance of RA in differentiation and fetal development these drugs are considered potential teratogens, which may cause fetal harm if significant absorption occurs in a woman who is pregnant.
First generation retinoids:
All-trans RA (ATRA, tretinoin), is the most abundant naturally occurring RA isoform. It is used to induce remission in acute promyelocytic leukaemia patients.
9-cis-RA (alitretinoin) is a naturally occurring endogenous retinoid used topically to treat severe chronic hand eczema refractory to potent topical corticosteroids. May be used in some countries to inhibit the growth of Kaposi’s sarcoma.
13-cis RA (isotretinoin) is primarily used to treat cystic acne, either topically or by mouth (under expert supervision).
Second generation retinoids:
Etretinate, was used to treat severe psoriasis, but was withdrawn from many markets due to the high risk of birth defects.
Acitretin, a metabolite of etretinate is used to treat severe extensive psoriasis resistant to other forms of therapy, palmoplantar pustular psoriasis, severe congenital ichthyosis and severe keratosis follicularis (Darier’s disease).
Third generation retinoids:
Tazarotene is used to treat mild to moderate plaque psoriasis affecting up to 10% of the skin area.
Bexarotene is used to cause regression of cutaneous T-cell lymphoma.
Adapalene is used to treat mild to moderate acne vulgaris.
Steroid hormones
Steroid hormones can be grouped into 2 classes: corticosteroids (typically made in the adrenal cortex) and sex steroids (typically made in the gonads or placenta).
Corticosteroids are subdivided in to the glucocorticoids (e.g. cortisol (=hydrocortisone) and cortisone; essential for metabolism of carbohydrates, proteins, and fats; anti-inflammatory activity) and the mineralocorticoids (principally aldosterone; maintenance of electrolyte and fluid balance). Corticosteroids are agonists of nuclear hormone receptors: glucocorticoids act via the glucocorticoid receptor and mineralocorticoids act via the mineralocorticoid receptor. These belong to a receptor family (3-ketosteroid receptors) which also includes the androgen receptor and progesterone receptor.
Sex steroids (or gonadal steroids) are those hormones which act via the androgen, estrogen or progesterone receptors (link to estrogen receptor family). Natural sex steroids are synthesized by the gonads, adrenal glands, or are converted from other sex steroids in the liver or adipose tissue.
Steroid hormones: source and functions
| Endocrine organ | Secreted hormone(s) | Effect(s) |
|---|---|---|
| Adrenal glands- cortex | glucocorticoids- zona fasciculata and zona reticularis cells | stimulates gluconeogenesis; stimulates fat breakdown in adipose tissue; inhibits protein synthesis and glucose uptake in muscle and adipose tissue; immunosuppressive; anti-inflammatory |
| mineralocorticoids- zona glomerulosa cells | stimulates active sodium reabsorption and passive water reabsorption in kidneys (increasing blood volume and pressure); stimulates renal potassium and H+ excretion | |
| androgens (secondary site of synthesis): DHEA and testosterone- zona fasciculata and zona reticularis cells | masculising effects in females; in males, effects are insignificant compared to those elicited by testicular androgens | |
| Adipose tissue | estrogens (mainly estrone)- adipocytes | |
| Reproductive organs- ovarian follicle and corpus luteum | progesterone- granulosa cells, theca cells | supports pregnancy |
| androstendione- theca cells | metabolic precursor of both testosterone and estrone | |
| estrogens (mainly estradiol)- granulosa cells | promotes development of secondary female sex characteristics; stimulates endometrial growth | |
| Testes | androgens, principally testosterone | virilizing action (prenatal and pubertal); anabolic action; spermatogenesis |
Corticosteroids in the clinic
Cortisol and synthetic corticosteroids are used widely as anti-inflammatory agents. Corticosteroids are available in different forms, including tablets, injectable forms, inhalation forms and topical lotions and creams. They are used to treat a huge variety of inflammatory conditions including asthma, allergic rhinitis and hay fever, urticaria, atopic eczema, chronic obstructive pulmonary disease (COPD), painful and inflamed joints, muscles and tendons, lupus, inflammatory bowel disease (IBD; including Crohn’s disease and ulcerative colitis) and multiple sclerosis (MS). In Addison’s patients corticosteroids are used as hormone replacement therapy.
Corticosteroids are prescribed at the lowest effective dose for the shortest possible time due to the long-term side-effects (e.g. weight gain, acne, thinning of the skin, osteoporosis, hypertension and diabetes).
Example corticosteroids
Betamethasone– for short-term topical treatment of local inflammation (eyes, skin), inflammatory and allergic disorders and asthma
Beclometasone– for similar indications as betamethasone
Clobetasone and clobetasol propionate– used topically to treat eczema, psoriasis and other forms of dermatitis. Clobetasone used in eye drops to treat dry eyes in Sjögren’s Syndrome.
Fluticasone– for asthma
Hydrocortisone (the approved name for cortisol)- used widely for mild inflammatory skin disorders such as eczemas.
Methylprednisolone– suppression of inflammatory and allergic disorders, treatment of local inflammation of joints and soft tissues, treatment of cerebral oedema associated with malignancy, treatment of graft rejection reactions,
Prednisolone– is widely used to suppress inflammatory and allergic reactions in a range of conditions including COPD (where increased breathlessness is interfering with daily activities), croup, acute asthma, idiopathic thrombocytopenic purpura, eczematous inflammation in otitis externa, ulcerative colitis, Crohn’s disease, rheumatoid arthritis, polymyalgia rheumatica and giant cell (temporal) arteritis.
Triamcinolone– intra-articular and peri-articular injection to treat local inflammation of joints and soft tissues
Aldosterone antagonists
Spironolactone is a potassium-sparing diuretic, which works by antagonising the effects of aldosterone. Used adjunctively to treat moderate to severe heart failure and resistant hypertension. Additional indicated conditions include Nephrotic syndrome, oedema in congestive heart failure, ascites in cirrhosis of the liver and malignant ascites.
Eplerenone works by the same mechanism as spironolactone. This drug is used adjunctively in heart failure patients with low left ventricular ejection fraction.
More information about these drug is contained in the Diuretics section of Cardiovascular system drugs.
Sex steroids in the clinic
The primary clinical use of testosterone is as hormone replacement therapy for males who produce sub-normal levels or no testosterone, which can cause hypogonadism. Testosterone production declines with age (the andropause). Testim®, Tostran® and Testogel® are testosterone medications used to treat hypogonadism due to testosterone deficiency.
Synthetic androgens are the anabolic steroids, often abused by athletes and other sportspeople to increase muscle strength and muscle mass, and possibly endurance. Nandrolone has been used clinically, but has been discontinued in the United States. It is approved in the UK to treat osteoporosis in postmenopausal women, but its use is not recommended.
Antiandrogens (or androgen receptor antagonists) are used to treat a variety of androgen-dependent conditions. In men they are most frequently used to treat prostate cancer, and also benign prostatic hyperplasia, and severe male sexual disorders (e.g. hypersexuality). In women they are used to reduce male hormone levels which cause hyperandrogenism and can be prescribed to treat acne, amenorrhea, seborrhea, hirsutism, androgenic alopecia, hidradenitis suppurativa.
Flutamide, nilutamide (not approved in the UK), bicalutamide and enzalutamide are non-steroidal antiandrogens. Combined androgen blockade and castration (orchidectomy) is used as a safe and effective prostate cancer therapy. Cyproterone acetate and abiraterone acetate are additional androgen receptor antagonists available to the prescriber. Abiraterone is primarily used in patients with metastatic castration-resistant prostate cancer.
5α-reductase inhibitors such as finasteride and dutasteride prevent the conversion of testosterone to dihydrotestosterone (DHT), so are indirectly antiandrogenic. 5α-reductase inhibitors are most often used to treat benign prostatic hyperplasia. The alpha-adrenoceotor antagonist tamsulosin can be used alongside 5α-reductase inhibitors to provide symptomatic relief in benign prostatic hyperplasia patients, as it acts to decrease urinary outflow resistance.
Progesterone receptor modulators
In the UK mifepristone is licensed to induce cervical ripening in preparation for mechanical termination of pregnancy procedures (up to 84 days gestation), to induce chemical termination of pregnancy (up to 49 days gestation; typically used with the prostaglandin E analogue misoprostol) or to induce labour in cases of fetal death in utero. Ulipristal acetate is used as emergency contraception (contained in the ellaOne morning after pill, which must be taken within 120 hours of sex) and for pre-operative and intermittent treatment of moderate to severe symptoms of uterine fibroids.
Synthetic progestogens (progestins) and estrogens are used in methods of hormonal contraception and to treat various reproductive and gynaecological conditions.
Progestins used in the clinic include:
Progesterone– used in assisted reproductive technology (ART) cycles to supplement the luteal phase and to treat infertility due to inadequate luteal phase, to provide progestogenic opposition of oestrogen HRT, and to treat premenstrual syndrome, dysfunctional menstrual bleeding and post-natal depression.
Medroxyprogesterone acetate is a long-acting progestin used in ‘depo’ contraceptives such as Depo-Provera®, given by injection every 12 weeks to maintain full protection. Such preparations can also be used to treat dysfunctional menstrual bleeding, secondary amenorrhoea, mild to moderate endometriosis, and to provide progestogenic opposition of oestrogen HRT. Medroxyprogesterone acetate is also used in treatment of endometrial, breast and renal cancers.
Etonogestrel– used in hormonal contraceptive implants (e.g. Nexplanon®) which are inserted subdermally into the lower surface of the upper arm and provide contraception for up to 3 years.
Norethisterone– a long-acting (8 weeks duration) progestin given by injection. It is used to stop bleeding in women with menorrhagia and dysfunctional menstrual bleeding, to treat endometriosis, dysmenorrhoea and premenstrual syndrome. Norethisterone can also be used to postpone menstruation and can be used in the treatment of breast cancer.
Desogestrel– used in hormonal contraceptives.
Megestrol acetate- used in the treatment of breast cancer.
Levonorgestrel– used in hormonal contraceptives, including as emergency contraception (e.g. Levonelle; one 1.5 mg dose taken as soon as possible after coitus, preferably within 12 hours but no later than after 72 hours). Levonorgestrel is the progestin used in progestogen-only intra-uterine devices such as Mirena®, Jaydess® and Levosert®. These IUDs are a good option for women with excessively heavy menses.
Synthetic estrogens
Synthetic estrogens are used clinically as a component of a large number of combined oral contraceptives, in estrogen replacement therapy for postmenopausal women, and hormone replacement therapy for trans women.
Ethinylestradiol is the most commonly used estrogenic compound contained in combined oral contraceptives. Estradiol (and its valerate salt) are also used in these birth control pills, as is mestranol (inactive prodrug of ethinylestradiol).
Serotonin
This topic is under construction. If you have relevant content you are willing to share, we would appreciate your contribution. Contact admin@pharmacologyeducation.org, or complete the webform on the Contribute to the Project page.
This is a recent review of the pathophysiological roles played by gasotransmitters in cancer and the potential of harnessing these agents as therapeutics. Table 1 provides an excellent overview of the sources, and chemical and biological properties of all three endogenous gasotransmitters.