This is a huge field of medicine. Our module covers those infections that represent large burdens on health care systems, and for which there are effective drug therapies.
If you have relevant content you are willing to share, we would appreciate your contribution. Contact admin@pharmacologyeducation.org, or complete the webform on the Contribute to the Project page.
Cytomegalovirus (CMV) infections
Human cytomegalovirus (hCMV, also known as human herpesvirus 5, HHV-5) is a common virus of the Herpesviridae family of viruses.
Infection is usually harmless and asymptomatic, but can cause glandular fever and pneumonia. It is spread through bodily fluids including saliva, semen, blood, urine, vaginal fluids and breast milk, and can be transmitted from mother to fetus during pregnancy resulting in congenital CMV infection. More than 90% of babies born with congenital CMV are asymptomatic, however a small proportion of these babies go on to develop some degree of hearing loss in their early years. If a high level of virus is transmitted to the fetus, the babies can be symptomatic from birth, and these babies exhibit range of symptoms and disabilities. Symptoms can include jaundice, pneumonia, purpura, hepatomegaly and splenomegaly, seizures, small size and small head size. Around 90% of babies with symptomatic congenital CMV from birth develop one or more physical or mental disabilities (e.g. hearing loss, visual impairment or blindness, learning difficulties, epilepsy, and lack of physical co-ordination). Congenital CMV can be treated with antiviral medicines such as ganciclovir (Cymevene), however treatment cannot cure a congenital CMV infection, and can only help to slow its progress.
There’s currently no vaccine for CMV.
Because CMV remains in the body for life, it can be re-activated. Both new infection or re-activation is a particular problem in patients who are immunocompromised or who are receiving immunosuppressant therapies, and in these patients infection can be life-threatening.
Cytomegalovirus Immune Globulin Intravenous (human) (CMV-IGIV) is an antibody-based therapy that has traditionally been used to manage CMV infection in organ transplant patients. CMV-IGIV can be used in combination with the antiviral agents ganciclovir, or its prodrug valganciclovir. Unfortunately, drug-resistant viral strains can emerge in patients treated with antiviral medications. Cidofovir is reserved for use in patients with ganciclovir-resistant infection. Foscarnet’s use is limited by its nephrotoxicity.
More about the drugs used to manage CMV infection, and their mechanisms of action, is available in our ‘Drugs for cytomegalovirus (CMV) infection‘ topic.
Genotypic resistance testing is being utilised to make more informed prescribing decisions, by determining the precise resistance mechanism acting in each patient. Sequencing the viral DNA polymerase UL97 and UL54 genes for resistance mutations can help to quickly determine the antiviral drug susceptibility phenotype present (Chevillotte et al., 2010, PMID: 19853628).
Malaria: prophylaxis and treatment
The learning resources at the bottom of this page provide links to reliable online materials that present current information about both the Plasmodium species responsible for malaria in humans, and the parasite’s lifecycle. These are useful as refreshers for learners.
Non-drug based interventions are effective and include bite-prevention strategies such as protective clothing, mosquito nets, vaporised insecticides and insect repellents that are applied to the skin.
Pharmaceutical treatment and prophylaxis of malaria relies on drugs that target the parasite at crucial stages of its lifecycle. Current drugs kill the asexual blood stage (a.k.a. erythrocytic forms, or schizonts) of the parasite in the blood, the primary and latent liver stages, or gametocytes.
The artemisinins (artesunate, artemether, lumefantrine), chloroquine, mefloquine, quinolones (quinine, quinidine), and antibacterial anti-malarials (pyrimethamine, sulfadoxine, doxycycline, clindamycin) all kill plasmodium parasites during the asexual blood stage.
Atovaquone + proguanil provides additional activity against the primary liver stages of P. falciparum.
Primaquine is effective against primary and latent liver stages as well as gametocytes, and it is most commonly used to eradicate the intrahepatic hypnozoites of P. vivax and P. ovale that are responsible for relapsing infections.
Prophylaxis and Treatment of Malaria
| Selecting appropriate drug or drug combination for prophylaxis or treatment is based on the susceptibility of the infecting parasite as determined by the geographical area where the infection was acquired. This map from the US Centers for Disease Control and Prevention (CDC) shows an approximation of the parts of the world where malaria transmission occurs. | 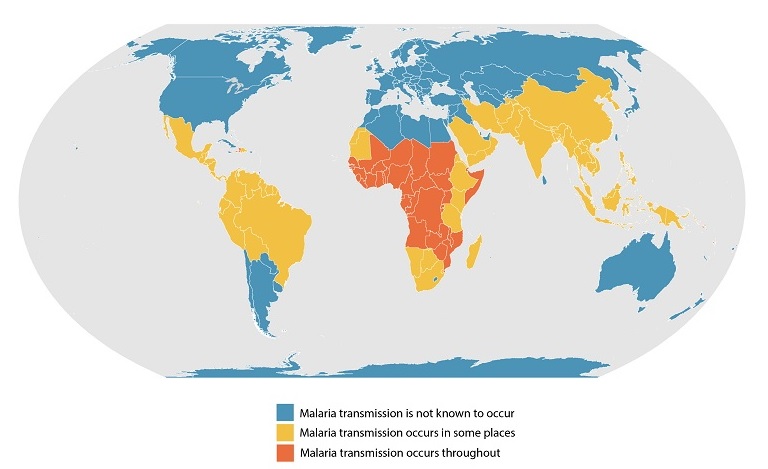 |
Drug based prophylaxis (chemoprophylaxis):
Short-term prophylaxis is recommended for residents from non-malarious countries who are travelling into areas where malaria is endemic. Best practice is to commence treatment before travel into a malaria zone, and to continue for a prescribed period of time after leaving the area.
The drugs used include chloroquine, mefloquine, atovaquone+proguanil and doxycycline. These drugs can be used for long-term prophylaxis and the choice of drug depends upon the extent of anti-malarial drug resistance in the destination area.
Treating Falciparum malaria (caused by Plasmodium falciparum):
All patients with Falciparum malaria should be admitted for hospital treatment, as there is a high risk of rapid deterioration, even once treatment has been initiated.
First-line treatment for uncomplicated Falciparum malaria is combination artemisinin drugs: Artemether with lumefantrine is the primary option, with artenimol with piperaquine phosphate as an alternative. Oral quinine or atovaquone + proguanil hydrochloride is suitable if an artemisinin combination is not available. Quinine is highly effective but poorly tolerated if treatment is prolonged, and this is usually prescribed in combination with oral doxycycline.
If the infection becomes severe or complicated, high dependency or intensive care is necessary, patients should be treated using Intravenous artesunate. If artesunate is temporarily unavailable, i.v. quinine can be administered until the artesunate arrives. If the patient responds to the initial artesunate, they should be switched to a full course of artemisinin combination therapy (oral quinine + doxycycline, or atovaquone + proguanil hydrochloride are suitable alternatives as described above).
Most P. falciparum is resistant to chloroquine, voiding its use. Due to concerns about adverse effects of mefloquine, the drug is used only when no other treatment options are available.
Treating non-falciparum malaria (caused by Plasmodium vivax, P. ovale, P. malariae, or P. knowlesi, dependent on geographic location):
The first-line options for P. vivax infections are artemisinin combination therapies, or chloroquine. Artemisinin combinations might offer better coverage in some regions due to chloroquine-resistant strains of P. vivax.
Because of its high activity against hypnozoites, primaquine is used for terminal chemoprophylaxis and radical cure of P. vivax and P. ovale infection.
RESOURCES
This webpage provides information about the species of Plasmodium that are recognised as causing malaria in humans around the globe. It is regularly updated.
This wepage provides links to an animated PowerPoint slide and short animated movies that describe the lifecycle of the Plasmodium parasite. It was developed in collaboration with the Medicines for Malaria Venture(MMV).
This specialist-curated webpage hosts a list of anti-malarial drugs which are currently, or have been in the past, approved for human clinical use by a regulatory agency.
HIV
HIV type 1 (HIV-1, HIV) infects CD4+ T cells of the immune system, via interactions with CD4 on T cell membranes and with the co-receptors CXCR4 and CCR5, which are two chemokine GPCRs. Once inside the cell the HIV genome is inserted into the host genome and hijacks the host transcriptional and translational machinery to replicate new viral particles. HIV infection ultimately leads to destruction of CD4+ T cells as the T cells lyse and release new virus, which go on to infect and destroy more T cells. The cumulative effect dramatically reduces the patient’s T cell population and therefore their ability to mount an effective response to further infections.
Treatment with anti-HIV medicines (antiretrovirals or ARVs) is called antiretroviral therapy (ART). The principal action of ART is to lower viral load and promote immune re-constitution and viraemic control, with the aim of reducing the risk of progression to AIDS.
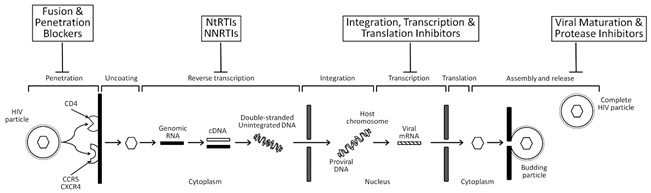
The ART drugs available target crucial and amenable steps in the life cycle of HIV infection and replication (see figure below). The FDA has approved more than two dozen antiretroviral drugs to treat HIV infection. A patient’s initial HIV regimen generally includes three HIV medicines from at least two of the different drug classes described below.
Nucleoside/Nucleotide Reverse Transcriptase Inhibitors (NRTIs)
NRTIs inhibit activity of reverse transcriptase, a viral DNA polymerase that is required for replication of HIV and other retroviruses. Viral reverse transcriptase copies the single stand of the HIV’s RNA genome creating a double-stranded viral DNA that is able to integrate into the host chromosomal DNA. Host transcription and translation are hijacked to reproduce the virus. This group of drugs are analogues of the host’s endogenous deoxynucleotides that are required to synthesize viral DNA, but when incorporated in to a growing DNA molecule they block further elongation, acting as chain terminators. Drugs of this type can be either nucleoside or nucleotide analogues, with the former requiring kinase-mediated phosphorylation to generate active triphosphate molecules. Nucleoside reverse transcriptase inhibitors were the first type of ART drugs to be developed.
Examples include:
Abacavir, or ABC (Ziagen)
Didanosine, or ddl (Videx)
Emtricitabine, or FTC (Emtriva)
Lamivudine, or 3TC (Epivir)
Stavudine, or d4T (Zerit)
Tenofovir, or TDF (Viread)
Zidovudine, or AZT or ZDV (Retrovir)
Non-nucleoside Reverse Transcriptase Inhibitors (NNRTIs)
NNRTIs bind directly to the viral reverse transcriptase and inhibit its activity. This action prevents viral replication.
Delavirdine (Rescriptor)
Efavirenz (Sustiva)
Etravirine (Intelence)
Nevirapine (Viramune)
Rilpivirine (Edurant)
Protease Inhibitors (PIs)
HIV protease inhibitors are peptidomimetics that competitively inhibit the action of the virus aspartyl protease, and enzyme crucial for the proteolytic cleavage of nascent polypeptide precursors into mature viral proteins.
Atazanavir, or ATV (Reyataz)
Darunavir, or DRV (Prezista)
Fosamprenavir, or FPV (Lexiva)
Indinavir, or IDV (Crixivan)
Lopinavir + ritonavir, or LPV/r (Kaletra)
Nelfinavir, or NFV (Viracept)
Ritonavir, or RTV (Norvir)
Saquinavir, or SQV (Invirase)
Tipranavir, or TPV (Aptivus)
Cobicistat (Tybost) is an adjuvant drug that increases atazanavir and darunavir efficacy, but it can cause life-threatening kidney problems if it is adminstered with certain other medicines.
Atazanavir + cobicistat, or ATV/COBI (Evotaz)
Darunavir + cobicistat, or DRV/COBI (Prezcobix)
These first three groups of drugs work at the level of the HIV infected cell to inhibit viral replication.
The next groups of drugs have different mechanisms of action.
Entry (or Fusion) Inhibitors
Drugs of this class block viral fusion and entry to the T cells.
Enfuvirtide, or ENF or T-20 (Fuzeon), is a biomimetic peptide that binds to the viral transmembrane protein gp41, and inhibits formation of the entry pore that is required for the capsid of the virus to enter the cell. Enfuvirtide is active against HIV-1, with very low activity against HIV-2. Enfuvirtide is delivered by injection, so adherence may be an issue for some patients.
In March 2018, the US FDA approved a first-in-class treatment for heavily treatment-experienced patients with multidrug resistant HIV. Ibalizumab-uiyk (proprietary name Trogarzo; IMGT link) is an anti-CD4 (CXCR4) monoclonal antibody that inhibits the viral entry process (see Jacobson et al. (2009)), and is able to block CCR5- and CXCR4-tropic viruses. Ibalizumab-uiyk is to be used in combination with an optimized background regimen of other antiretroviral drugs.
CCR5 Antagonist
Drugs with this action are also entry inhibitors, but with a distinct mechanism of action compared to enfuvirtide. The CCR5 chemokine receptor is an important co-receptor that HIV-1 uses to attach to cells before viral fusion and entry into host cells. Maraviroc (MVC, Selzentry) is a CCR5 antagonist that inhibits the HIV-CCR5 interaction and thereby prevents HIV from entering the cells. Many treatment-experienced patients may have non-CCR5-tropic virus. Thus, screening patients with tropism assays (e.g., Trofile) before maraviroc initiation is essential.
Integrase Inhibitors (or integrase strand transfer inhibitors (INSTIs))
Integrase is a key viral enzyme that facilitates integration of retroviral DNA into the host cell genome. Drugs of this family inhibit this process, thereby preventing viral replication.
Dolutegravir (Tivicay)
Elvitegravir (Vitekta)
Raltegravir (Isentress)
Cabotegravir (Vocabria)
Attachment Inhibitors
This new class of HIV drugs blocks viral attachment to the host CD4 molecule on T-lymphocytes.
Fostemsavir was the first example of this class to be approved by the FDA (in 2020). It is indicated for HIV infections that cannot be successfully treated with other ARTs because of resistance, intolerance or safety considerations.
Capsid Inhibitors
Drugs with this mechanism of action block capsid protein oligomerization and disrupt interactions with host factors that are crucial for both early and late phases of the viral replication cycle. Lenacapavir was the first drug of this class to be approved for clinical use (in 2022, by the EMA & FDA). It is a long-acting drug that’s administered as a subcutaneous depot injection, once every 6 months. It is prescribed in combination with other antiretrovirals. Like Fostemsavir, lenacapavir’s use is reserved for HIV infections that cannot be successfully treated with other ARTs because of resistance, intolerance or safety considerations.
Fixed-Dose combination HIV medications
Abacavir + dolutegravir + lamivudine, or ABC/DTG/3TC (Triumeq)
Abacavir + lamivudine, or ABC/3TC (Epzicom)
Abacavir + lamivudine + zidovudine, or ABC/3TC/ZDV (Trizivir)
Efavirenz + emtricitabine + tenofovir, or EFV/FTC/TDF (Atripla, Tribuss)
Elvitegravir + cobicistat + emtricitabine + tenofovir, or EVG/COBI/FTC/TAF or ECF/TAF (Genvoya)
Elvitegravir + cobicistat + emtricitabine + tenofovir, or EVG/COBI/FTC/TDF or ECF/TDF (Stribild)
Emtricitabine + rilpivirine + tenofovir, or FTC/RPV/TAF (Odefsey)
Emtricitabine + rilpivirine + tenofovir, or FTC/RPV/TDF (Complera)
Emtricitabine + tenofovir, or TAF/FTC (Descovy)
Emtricitabine + tenofovir, or TDF/FTC (Truvada)
Lamivudine + zidovudine, or 3TC/ZDV (Combivir)
Cabotegravir + rilpivirine (Cabenuva; co-packaged) is a once monthly injectable regimen for uncomplicated infections.
ART adherence is essential to prevent drug-resistant strains of HIV developing. If ART is used properly HIV-positive patients can now live long, active lives.
Prescribing decisions are reached by considering existing medical conditions, immune system function, and should involve discussions about which regimen the patient would prefer, and would be most likely to adhere to.
Pre-exposure prophylaxis (or PrEP) is the most recent advance in ART, with the approval of Truvada as a therapy to reduce the likelihood of HIV infection in high risk individuals (e.g. to reduce the risk of HIV-negative people getting HIV from a sexual or injection-drug-using partner who is HIV-positive). The CDC (https://www.cdc.gov/hiv/basics/prep.html) reported that among people who inject drugs, PrEP reduces infection risk by >70%. If combined with ‘safe sex’ the risk of getting sexually transmitted HIV whilst taking PrEP is reduced by up to 90%.
Continuing care
CD4 count (every 3-6 months)
Viral load (every 3-4 months)
HIV strain tests to ensure a resistant form hasn’t appeared that would stop drugs from being effective.
Cholesterol and triglyceride tests, because HIV and many of the antiretroviral drugs that treat it can raise the levels of these fats
Checks for infections including STIs, and opportunistic infections such as pneumonia, Salmonella, candidiasis, hepatitis, tuberculosis and toxoplasmosis.
Ensuring vaccinations are up to date to prevent diseases such as chicken pox, measles, mumps, influenza, and polio. HIV positive patients can receive anti- pneumonia vaccines.
Ongoing Drug Development
Drugs with alternative modes of action are being sought to overcome the problems associated with acquired drug-resistance.
For example, PRO 140 is a humanized monoclonal antibody targeted against the CCR5 receptor. In Phase 3 clinical trial.
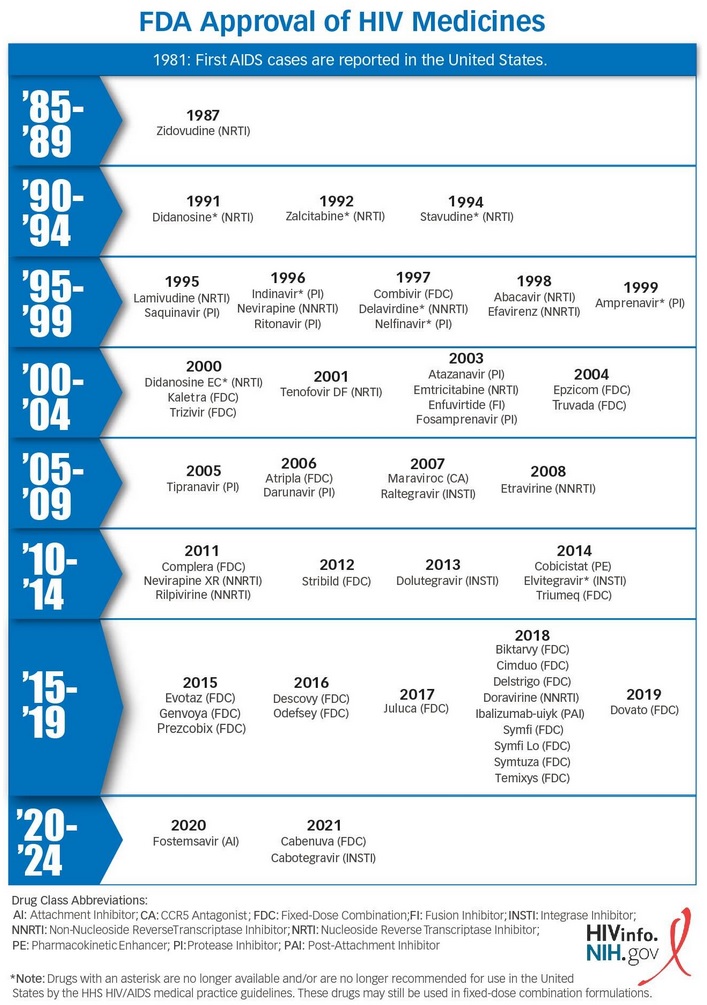
The infographic below presents a timeline of HIV drug approvals by the US FDA (https://hivinfo.nih.gov/understanding-hiv/infographics/fda-approval-hiv-medicines)
RESOURCES
This is an immunology website based in South Africa, in partnership with the International Union of Immunological Societies (IUIS), that has a strong emphasis on HIV and AIDS. The website offers Teaching and Learning Tools (including core immunology modules) as well as a Treatment & Diagnostics section that includes HIV-specific topics such as HIV Life Cycle, Declining CD4 count and ARV Drug Information.
This fact sheet provides a detailed and up-to-date list of FDA approved HIV ARVs, grouped by mechanism of action. Links to more detailed pages for each drug are provided. Suitable for intermediate learners.
Accessed from aidsinfo.nih.gov in August 2017.
Viral hepatitis
There are five known hepatitis viruses: A, B, C, D, and E. All cause disease which primarily affect the liver.
Hepatitis A
Hepatitis A is an infectious disease caused by the hepatitis A virus (HAV). Hepatitis A is common in regions of the world with poor sanitation and inadequate safe water sources. Transmission routes are faecal-oral and blood. HAV infection is often asymptomatic, but when they do occur symptoms may include nausea, vomiting, diarrhoea, jaundice, fever, and abdominal pain. Acute liver failure is a rare complication that is more common in the elderly.
Infection can be prevented by vaccination. Resistance is life-long following a single natural infection.
There is no specific treatment for HAV infection, other than maintaining adequate nutritional balance, and fluid replacement if vomiting and diarrhoea are severe.
Hepatitis B
Hepatitis B is an infectious disease caused by the hepatitis B virus (HBV). It can cause both acute and chronic infections. Most cases of chronic disease are asymptomatic, however, cirrhosis and liver cancer may eventually develop. HBV is transmitted by exposure to infectious blood or body fluids. The infection can be diagnosed 30 to 60 days after exposure. HBV infection has been preventable by vaccination since 1982, with two or three doses required to achieve full protection. Natural life-long resistance develops following infection.
During initial infection, care is based on the patient’s symptoms. As an exception, early antiretroviral therapy may be indicated for cases of aggressive (fulminant) hepatitis or when the patient is immunocompromised. In those who develop chronic disease, antiviral medication such as tenofovir or interferon may be useful to reduce the risk of cirrhosis and liver cancer. The drugs available cannot clear the infection, rather they inhibit viral replication to limit liver damage. The World Health Organization recommended a combination of tenofovir and entecavir as first-line agents.
Drugs for HBV infections are discussed in more detail in the topic ‘Viral hepatitis- HBV and HBC‘
This review, published in The Lancet in Feb 2023 (doi.org/10.1016/S0140-6736(22)01468-4), contains a huge amount of detailed information about HBV, including synopses of current therapies, and of some new antiviral and immunomodulatory therapies that are in clinical development. It is hoped that some of these new agents will rid the body of HBV antigens and achieve a ‘functional cure’ of HBV infection.
Hepatitis C
Hepatitis C is an infectious disease caused by the hepatitis C virus (HCV). Few symptoms are evident during the initial period of infection, or even when disease has progressed to early chronic infection. Damage accumulates over time and can lead to liver disease, cirrhosis and liver cancer. HCV is spread primarily by blood-to-blood contact (e.g. associated with intravenous drug use, poorly sterilized medical equipment, needlestick injuries in healthcare, blood transfusions, and mother-to-child transmission).
There is no vaccine against hepatitis C, however chronic HCV infection can be effectively managed about 95% of the time with antiviral medications. HCV treatment focusses on management rather than cure. Treatment aims are:
- eradication of virus
- decreasing morbidity and mortality
- normalization of biochemical markers
- improving clinical symptoms
- preventing spread of the disease
- preventing progression to cirrhosis and hepatocellular carcinoma
- preventing the development of end-stage liver disease and its manifestations
Drugs for HCV infections are discussed in more detail in the topic ‘Viral hepatitis- HBV and HBC‘
There are at least six genetically distinct HCV genotypes, or strains. Knowing the strain of the virus can help inform treatment recommendations. Treatment during the first six months is more effective than once chronic infection has established. In the US population, it is estimated that ~75% of HCV infections are genotype 1; 20-25% are genotypes 2 or 3; and the remaining small number of infections are genotypes 4, 5 or 6.
HCV genotypes
| HCV genotype | Recommended treatment regimen | Alternative treatment regimen |
| 1a | 12 weeks of ledipasvir + sofosbuvir | 12 to 24 weeks of paritaprevir + ombitasvir + dasabuvir + ribavirin |
| 1b | 12 weeks of ledipasvir + sofosbuvir | 12 weeks of paritaprevir + ombitasvir + dasabuvir |
| 2 | 12 to 16 weeks of sofosbuvir and ribavirin | |
| 3 | 12 weeks of sofosbuvir + ribavirin + pegylated interferon | |
| 4 | 12 weeks of ledipasvir + sofosbuvir or paritaprevir + ritonavir + ombitasvir + ribavirin | 24 weeks of sofosbuvir + ribavirin |
| 5 or 6 | sofosbuvir + ledipasvir | |
|
Recommendations based on AASLD/IDSA HCV Guidance, Panel (September 2015). PMID 26111063
|
||
Hepatitis D
Hepatitis D is caused by the hepatitis D virus (HDV), a small spherical enveloped viroid, which can only replicate if co-infected with HBV. The presence of HDV+HBV results in more severe complications compared to infection with HBV alone, including greater risk of developing liver failure during acute infection, more rapid progression to cirrhosis and an increased risk of chronic infection progressing to liver cancer. HBV+HDV infection has a fatality rate of ~20%, the highest of all hepatitis infections. HDV infection is rare in developed countries, where it is mainly restricted to groups at high risk of hepatitis B infection, especially injecting drug users and to a lesser extent, patients receiving clotting factor concentrates.
Because of its reliance on HBV for replication, anti-HBV vaccination is HDV preventative. Pegylated interferon alpha is effective in reducing hepatitis D viral load, but it increases again when treatment is discontinued.
Hepatitis E
Hepatitis E is caused by the hepatitis E virus (HEV). HEV has a faecal-oral transmission route. Infection is usually acute and self-limiting, with low mortality in developed countries. However, immunocompromised patients (in particular organ transplant recipients taking immunosuppressive drugs) are at a greater risk of developing chronic HEV hepatitis, and these patients have a higher mortality rate. HEV infection is fatal in only ~2% of all cases. One other group with increased mortality (up to ~20%) is pregnant women who can develop a clinical syndrome called fulminant liver failure when infected with HEV.
Sanitation is the most important measure in prevention of HEV infection. The HEV 239 vaccine is available in China, but the WHO does not make a recommendation regarding its routine use.
In terms of drug treatment, there is off-label experience for treating chronic hepatitis E infection with ribavirin, which indicates that low dose ribavirin for 3 months is associated with viral clearance in about two-thirds of chronic HEV infections. Virus can be cleared in organ transplant patients by temporarily reducing their level of immunosuppression.
This webpage provides information about the species of Plasmodium that are recognised as causing malaria in humans around the globe. It is regularly updated.